Category AMS strategy

Giving and taking advice – how to get great antibiotic care for your patients
Guest posting from Dr Catherine Berry, Infectious Diseases Staff Specialist and Antimicrobial Stewardship lead for Hunter New England Health. I’m still recovering from a week of ID on call. It’s intense and we provide service for a huge area of NSW. It’s interesting and challenging trying to see the problem through the referrer’s eyes. Some […]
Antimicrobial resistance awareness week 2023 – short presentations
Presented between November 18-24th : Oral is the New IV presented by Professor Josh Davis and Ms Kristi Kozierowski (AMS pharmacist, John Hunter Hospital): Oral is the New IV_JHH Davis 2023 Oral is the new IV – 2023 – KK Antibiograms presented by Dr Rob George (Microbiologist, Pathology NSW) Are we looking after our antibiotics in Hunter […]
Updated overview of approaches to CRE/ CPE treatment
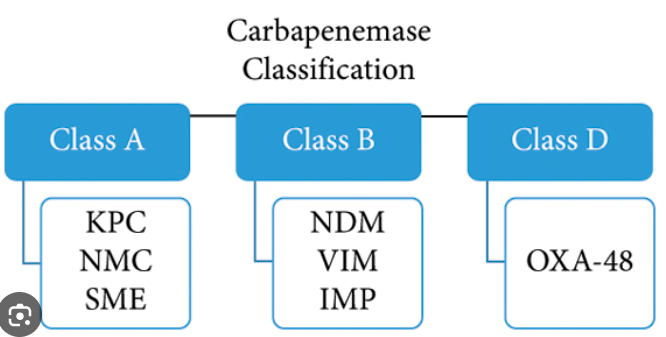
Guest posting from Professors Josh Davis (Hunter New England Health) and Patrick Harris (UQ). AMBLER CLASS Class A Class B Class D Key characteristic Serine group enzyme Metallo-betalactamase OXA-type Key example(s) KPC, GES IMP, NDM, VIM OXA-48. (OXA-181, OXA-232 emerging) Susceptiblity features R to all b-lactams R to all b-lactams except Aztreonam May harbour other […]
Antibiotic Awareness Week 2022 – short seminar links x4
Here are the presentations from our recent short AMS lectures for AAW! AMS- Who the blood hell are ya? Holly Jordan Jordan AAW Nov22 Overview of AMS at JHH Shorter is Better. Josh Davis Davis Nov22 AAW slides Shorter is better Choosing antibiotics wisely – who really needs ceftriaxone or pip/tazo? John Ferguson Ferguson AAW Nov22 […]

Chronic venous or dependency wound golden rules
Guest posting from Dr Nicole Organ, Vascular Surgeon, HNE LHD Golden rules Maintain lower limb skin integrity – trauma avoidance, protective routine skin care Treat acute lower limb wounds/skin tears aggressively to prevent chronicity – early use of wound compression Address modifiable risk factors – superficial venous disease, obesity, sedentary lifestyle, arterial disease Use simple […]

Why does our local CAP guideline differ from Australian Therapeutic Guidelines?
Kristi, Lorrae and Ayesha have recently joined as AIMED authors– welcome aboard. Here’s a posting from Kristi that unpacks the approach to community-acquired pneumonia (CAP) in Hunter New England Health, NSW. In adults, the most common bacterial cause of community-acquired pneumonia (CAP) is Streptococcus pneumoniae. Other pathogens associated with CAP include Haemophilus influenzae and atypical’ […]

How long should that antibiotic course last?
Guest posting from Ms Kristi Kozierowski, AMS and ICU pharmacist, John Hunter Hospital, NSW, Australia. This is a useful evidence-based summary produced for AAW 2019 – Duration FINAL Kozierowski 2019. Usage welcome with acknowledgement. References Shorter is better : evidence review by Brad Spellberg

Acute piperacillin+tazobactam shortage – important advice – JHH and HNELHD
Currently (still in Feb 2018) there is a worldwide shortage of piperacillin+tazobactam , an additional issue to the shortage earlier in 2017 . Appropriate substitutions – see – HNELHD advice (November 2017) JHH_Pip_Taz_Fact_Sheet_Oct_2017 . This includes new dosage recommendations for IV amox+clavulanate for intra-abdominal infection (6 -hrly rather than 8- hrly dosing). For further advice, please contact the […]
Overuse => global shortage! Let’s conserve what piperacillin+tazobactam we have left
Piperacillin+tazobactam (Tazocin) is one of our most important broad spectrum agents and is in short supply. Please conserve it by avoiding use in these common situations: Uncomplicated biliary sepsis (Use ampicillin+gentamicin(max 48hrs) OR if allergic, ceftriaxone) Urinary tract infection with sepsis (Use ampicillin+gentamicin(max 48 hrs) OR if allergic, ceftriaxone) Early onset (< 5d after admission) […]
Q3 Tragedy of the commons and antimicrobial stewardship
Question 3 of our JMO pre-test survey asked about the aims of antimicrobial stewardship (yes, better ‘antimicrobial’ than ‘antibiotic’- antiviral, antifungal, antiparasitic resistance are issues as well). We gave you three options and all except one responded with the correct answer – all three! The order is important – treatment of the individual patient comes first: Optimise the effectiveness […]
