Author Archives: mdjkf
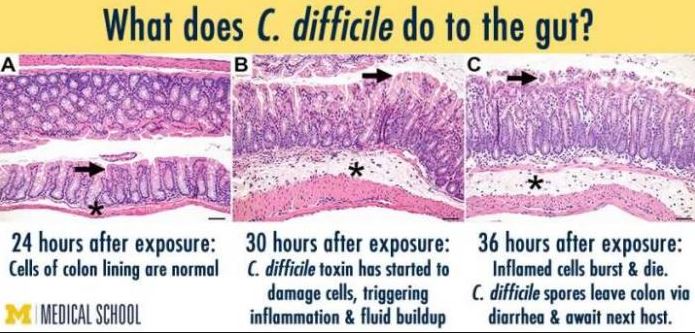
Clostridium difficile – misconceptions about testing
Confine testing to symptomatic patients. Testing of patients with formed stools may generate false positives due to asymptomatic carriage of toxigenic strains. An unfortunate side effect of multiplex PCR stool assays, are that tests that are inappropriate to the clinical circumstance may be performed, generating false positives. Also test at-risk (i.e. antibiotic or ppi-exposed) symptomatic […]

Reducing ESBL Gram negative fluoroquinolone resistance – what is the ecological sweet spot for usage?
This excellent recent paper from Sarma et al brings focus on what the target level of quinolone use should be in order to have an impact on quinolone resistance in Enterobacteriaceae. It describes the situation across a region of England (9 hospitals and other facilities) where quite stringent control of cephalosporin use was already in place […]

Bronchiectasis and goals of antibiotic treatment – thinking it through
The setting – patients with bronchiectasis (including those with cystic fibrosis) have impaired respiratory secretion clearance and a vastly different lower respiratory flora (microbiome) than patients with normal lungs. They are frequently colonised with conventional respiratory species such as Haemophilus influenzae and Moraxella catarrhalis, Staphylococcus aureus, a diverse range of Gram negative bacteria and even fungi. Colonisation/infection with non-tuberculous […]
Inducing ceftriaxone-deficiency in hospitals: practical stewardship insights
2018 update! Just as relevant. Upside – Ceftriaxone and cefotaxime (third generation cephalosporins-TGC) are amongst the most important agents for directed therapy of infections due to Gram negative organisms that are resistant to ampicillin or cephazolin (a first generation cephalosporin), including Klebsiella pneumoniae . They penetrate the CSF well, making them important agents for treatment of meningitis due to […]
Why do Gram positive and Gram negative bacteria show different antibiotic susceptibility patterns?
The terms Gram positive and Gram negative are commonly used to describe bacteria. The main difference between the two is the structure of their cell wall which changes their susceptibility to different antibiotics. The separation also loosely fits the location of these organisms in the body – Gram negative organisms predominate in the bowel (eg. […]
Tazocin misconceptions: misuse in community-acquired pneumonia – spectrum too broad
Piperacillin+tazobactam (Tazocin) is an important broad spectrum antibiotic that is still active in most Australian settings against a wide range of Gram negatives (including Pseudomonas) , Gram positives (excluding MRSA and VRE) and nearly all anaerobic bacteria. It comes into great demand for management of a range of healthcare-associated infections, especially in ICU. Its use […]
Aids to structuring antimicrobial stewardship rounds and improving documentation
We’ve used the following aids at John Hunter Hospital for some years which others are very welcome to adopt/adapt:
Case report: Community-Acquired Pyelonephritis in Pregnancy Caused by KPC-Producing Klebsiella pneumoniae
In northern NSW, we already face cases similar to that described below – infection with multi-drug resistant carbapenemase-producing Gram negative organisms. The major global types of these organisms are named with acronyms that refer to the type of carbapenemase gene – KPC, NDM (New Delhi Metallobetalactamase), IMP (imipenemase) and others. KPC-type organisms are prevalent in Greece, […]
Choosing wisely (IDSA): Avoid antibiotic therapy for lower limb stasis dermatitis or venous ulcers
The Infectious Diseases Society of America also has started a Choosing wisely campaign. This advice is valuable. In the recent District-wide wound surveillance survey across Hunter New England Health hospitals and community nursing services, there were over 900 patients with active wounds identified (including many venous ulcers related to stasis dermatitis). Of these 28% had received antibiotics in […]
Ten infection prevention commandments for medical staff
Thanks Craig Boutlis who helped me develop these some time back. Nothing has changed much yet! Always disinfect your hands with alcohol-based hand rub BEFORE and AFTER touching a patient or performing a procedure. Set the example for your team and expect others to follow your lead. Dress well for safer care – abandon ties […]
